
An Update on Equine Cushing’s Disease
Equine Cushing’s Disease or pituitary pars intermedia dysfunction (PPID) is the most common endocrine disorder of horses. This disorder develops secondary to degeneration of neurons extending from the hypothalamus (the body’s hormone control center) to the pituitary gland (a major hormone release gland). These neurons should normally regulate the release of hormones from the pituitary gland and so lack of this inhibition overtime results in growth and secondarily increased hormone production from the pituitary gland. Neoplasia develops over time in the form of functional pituitary adenomas (a benign cancer). These tumors secrete large amounts of hormones including ACTH affecting system throughout the body.
The prevalence of PPID increases with age. Approximately 20% of equids (horses, donkeys, and mules) over 15 years and 30% of equids over 30 years of age are affected by the disease. Clinical signs can be obvious in advanced disease (long hair coat, poor shedding, laminitis, muscle wasting, immune compromise) but may be more subtle in its earlier stages (mild muscle atrophy, delayed healing, infertility, increased urination/drinking). Treatment of the disease involves life-long management with a medication (pergolide) and management changes but if managed appropriately, horses with PPID can have an excellent quality of life.
Diagnosis of PPID: The first-line test when PPID is suspected is a blood ACTH test. This is an excellent test during later stages of disease progression but does not always catch horses early on in the disease process.
If there is strong suspicion for PPID and a horse has “equivocal” blood results after a baseline ACTH test then a treatment trial with Prascend may be recommended.
In horses where a definitive diagnosis is desired, a TRH stimulation test can be performed.
For this test, the horse will have a baseline ACTH pulled and then be administered an intravenous dose of a hormone called TRH. Exactly 10 minutes later, blood is pulled again for a post-TRH ACTH analysis.
For horses with PPID, even early in the course of disease, their post-TRH ACTH value will be markedly elevated compared to a normal horse.
If equine metabolic syndrome (EMS) is also suspected, then bloodwork for that may be pulled at the same time (see last week’s blog for more information).
Note on seasonality: Reference ranges for normal ACTH are seasonally dependent and so repeat testing should take this into account. Because of this seasonal nature, TRH stimulation tests are most useful for identifying early cases of PPID from January through June.
Treatment of PPID: Most successful treatment of PPID is with the medication Prascend (pergolide). This is a medication that is given by mouth once daily for life. It is essential for mitigating the effects of PPID but is not considered curative (i.e. the disease can still progress with age).
Dose adjustment may be required as the horse ages and the disease progresses based on repeat blood testing and clinical signs.
For refractory cases, additional medication may be considered with veterinary guidance.
In horses with EMS, additional medications for insulin dysregulation may be considered (see last week’s blog for more info).
Wellness Care: In addition to medical management, horses with PPID should receive regular wellness care. Special attention should be paid to body condition, hoof care, dentistry, and parasite control as these can all be adversely affected in horses with undercontrolled PPID.
Diet: Appropriate management of weight and body condition is essential for horses with PPID. Feed selection should be based on their body condition score and any previously diagnosed insulin dysregulation (EMS).
For lean horses with normal insulin status, senior feeds and pasture grazing may be appropriate in addition to other feeds or supplements for weight and muscle gain pending your veterinarian’s recommendation.
Overweight horses or horses with insulin dysregulation should be put on restricted diets with low starch/sugar to help minimize the risk of laminitis as per your veterinarian’s recommendation.
Horses with increased thirst and urination should have adequate water available to them.
Note: Some dietary supplements have been suggested for the management of PPID but to date scientific evidence for their use is lacking.
Monitoring: Once treatment is started, or following changes in management, repeat testing will be recommended within 1-3 months.
For horses with consistent management, repeat examination and testing every 6-12 months (or sooner if concerns arise) helps to ensure that the PPID is well managed as the horse ages and the disease progresses.
Because of the seasonality around ACTH concentrations, it is recommended that repeat tests occur around the same time each year for most specific comparison of hormone values.
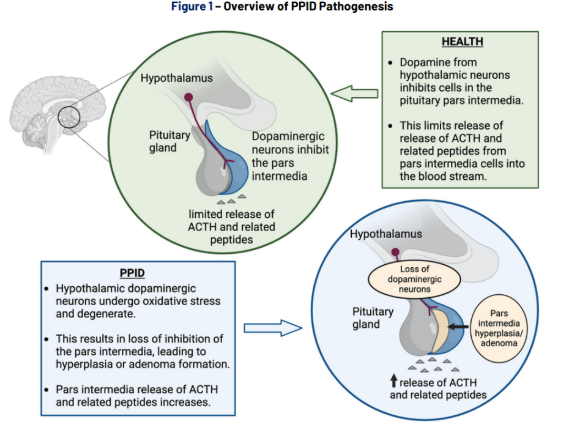
Image 1- Pathophysiology of PPID

Image 2- Signs of PPID can vary from long-hair coat (hypertrichosis) and being overweight (often when EMS is also present) to delayed or patchy shedding and muscle loss.
Reference: Equine Endocrinology Group 2023 Recommendations on PPID.
https://static1.squarespace.com/static/65296d5988c69f3e85fa3653/t/6596d092174c8f1c3ae122b2/1704382615558/2023+EEG+PPID+-+Digital+version+with+insert+-+12.22.2023.pdf